American Medical Association’s Topline Summary: 2026 Medicare Physician Fee Schedule (MPFS) Final Rule
On October 31, 2025, the Centers for Medicare & Medicaid Services (CMS) releasedthe final rule for the 2026 Medicare physician fee schedule (MPFS). The AMA submitted detailed commentsto CMS regarding its proposals on Sept. 11, 2025. While the AMA staff analyze and develop a detailed summary of the more than 2,000-page rule, we want to bring a handful of key issues to your immediate attention.
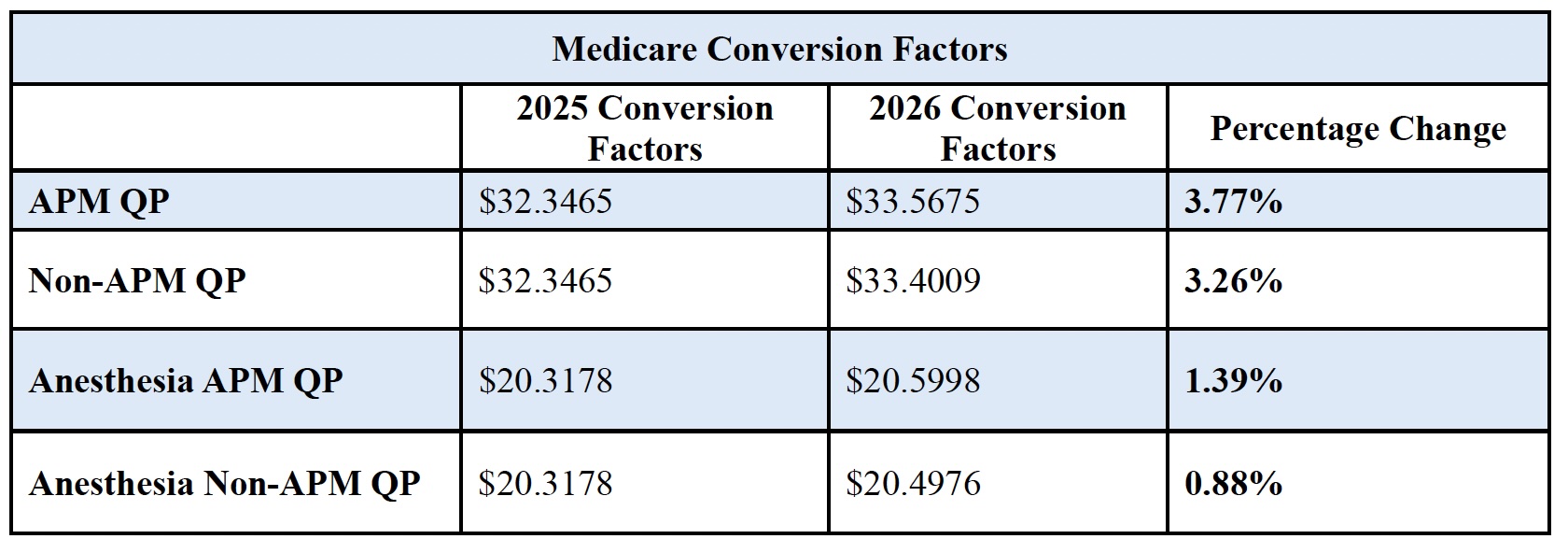
Conversion Factors and Budget Neutrality
For the first time this century, CMS finalized four conversion factors. The conversion factors reflect two different, small permanent updates to the baseline beginning January 1, 2026, as required under the Medicare Access and CHIP Reauthorization Act (MACRA) of 2015. Under MACRA, physicians who are qualifying participants (QPs)in advanced alternative payment models (APMs) will receive a somewhat higher conversion factor update and, thus, higher Medicare payments in 2026 compared to physicians who are not QPs. Each conversion factor also reflects the temporary, one-year 2.5 percent update enacted in H.R. 1.
Additionally, the conversion factors are affected by a positive .49 percent budget neutrality adjustment resulting from misvalued code changes and a -2.5 percent “efficiency adjustment.” Although AMA comments raised several questions about the proposed efficiency adjustment and recommended alternative approaches to achieve CMS’ objectives, CMS will apply the negative adjustment to work relative value units (RVUs) and the corresponding intra-service portion of physician time of non-time-based services that CMS believes accrue gains in efficiency over time. CMS will exempt new codes in 2026. This efficiency adjustment impacts most surgical specialties, radiology, and pathology by reducing their overall payment.
Of note, CMS accepted 90% of the AMA/Specialty Society RVS Update Committee’s (RUC’s) relative value recommendations for 2026.
Congress passed a temporary, one-year 2.5 percent update for 2026 in H.R. 1. The AMA continues to strongly advocate for permanent baseline updates to the conversion factors that
account for the growth in physician practice costs, which CMS projects will be 2.7 percent as measured by the MEI. In their
June 2025 Reportto Congress, the Medicare Payment Advisory Commission (MedPAC) expressed concerns about the growing gap between physicians’ input costs and Medicare payment, warning: “[t]his larger gap could create incentives for clinicians to reduce the number of Medicare beneficiaries they treat, stop participating in Medicare entirely, or vertically consolidate with hospitals, which could increase spending for beneficiaries and the Medicare program.” MedPAC therefore recommended Congress repeal current law updates and replace them with annual updates tied to MEI for all future years. The2025 Medicare Trustees Reportreiterated similar concerns about patient access to care, stating that under current law, “the Trustees expect access to Medicare-participating physicians to become a significant issue in the long term.”
Practice Expense
The AMA is disappointed that CMS did not factor in the Physician Practice Information (PPI) Surveyinformationin updating 2026 practice expense relative values to adjust Medicare Economic Index (MEI) weights impacting the distribution of RVU components. Independent from the PPI Survey, CMS chose to finalize its proposed modification to the indirect practice expense methodology, redistributing indirect practice costs from facility-based services to non-facility-based services. This change in practice expense methodology, only recognizing 50 percent of the physician's work of facility-based services in the indirect cost method, results in a dramatic shift of payment between sites-of-service. Facility-based payment to physicians will decrease overall by -7 percent while non-facility-based payment to physicians will increase by 4 percent, but reductions for specific physician practices will be even steeper.
Telehealth
The AMA is extremely concerned that the ongoing government shutdown has led to a lapse in Medicare telehealth flexibilities that had been in place since 2020, except for telehealth services for patients with a mental health condition or substance use disorder. This lapse demonstrates more than ever the need for Congress to pass legislation permanently enabling Medicare patients to obtain telehealth services all over the country, not just in rural areas, and to be able to get telehealth services delivered to them at their home without having to travel to a medical facility.
Nonetheless, the AMA is pleased that for 2026 CMS is finalizing its proposals, long advocated by the AMA, to permanently lift the frequency limits on telehealth services provided to patients in hospitals and skilled nursing facilities and permanently allow virtual direct supervision for most services that require supervision. The AMA is also pleased that CMS agreed with AMA and other commenters to continue the policy currently in place allowing teaching physicians to provide virtual supervision to residents providing telehealth services in all training sites and not limit this policy only to rural areas.
Merit-based Incentive Payment System (MIPS)
Following ongoing advocacy by the AMA, we are pleased that CMS maintained the performance threshold to avoid a MIPS penalty of up to 9 percent at 75 points for the CY 2026 performance
year/2028 MIPS payment year through the CY 2028 performance year/ 2030 MIPS payment year. The stability with the performance threshold should provide physicians with more of an opportunity to earn a positive or neutral incentive.
Unfortunately,researchcontinues to show that MIPS is unduly burdensome; disproportionately harmful to small, rural, and independent practices; exacerbating differences in care for patients with social risk factors; and divorced from meaningful clinical outcomes. In 2025, 14 percent of all MIPS-eligible clinicians are subject to a penalty of up to -9 percent of their Medicare paid amount for covered services as a result of MIPS. By comparison, 29 percent of small practices, 49 percent of solo practitioners, and 18 percent of rural practices are receiving a MIPS penalty. Worse, 13 percent of small practices and 29 percent of solo practitioners are receiving the maximum MIPS penalty of -9 percent. The AMA isstronglyurging Congress to make statutory changes to improve MIPS and address fundamental problems with the program by replacing steep penalties that disproportionately hurt small and rural practices and prioritize access to timely and actionable data.
Mandatory Payment Model
CMS finalized the Ambulatory Specialty Model (ASM) as proposed for implementation in 2027, a mandatory model for physicians in select specialties and geographic areas who treat patients with heart failure or low back pain. ASM is intended to encourage better collaboration between specialists and primary care physicians to prevent exacerbations and avoidable surgical procedures and hospital admissions. ASM performance will generate payment adjustments starting in 2029 of up to +/- 9 percent for the physicians who would be mandated to participate in it, rising to +/- 12 percent by 2033.
Additional resources
